A personal cardiology history
In the spring of 2006, at the age of 45, I began to have symptoms of severe unstable angina. However, I did not know what it was and I thought I had just pulled some muscles in my chest, or hurt my sternum. By August, I found I had to keep stopping when walking short distances due to the pain, which although not severe, was enough to make me rest. I went to my GP and he referred me to a cardiologist.
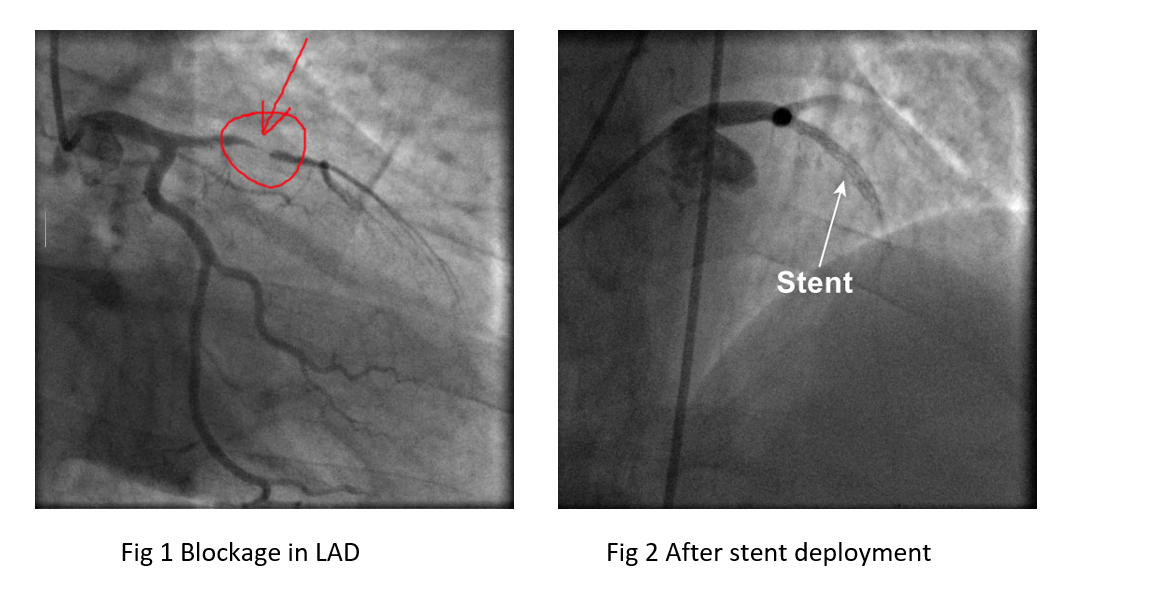
I had private health insurance with my employer, so I was seen privately within two weeks, on 20 September 2006. When he put me on an ECG for an exercise test, my readings were abnormal, and they suggested I had already had a heart attack. He arranged an angiogram with the option to proceed to angioplasty for the next morning. They found my left anterior descending coronary artery (LAD) was almost completely blocked and a heart attack was imminent. They cleared the blockage by deploying a stent and this ‘cured’ me. A few weeks later my ECG was normal, so my cardiologist decided that I had not had a heart attack previously.
In 2011, I began to have similar symptoms again and an angiogram in May revealed that the area below my stent was narrowing, and so he put another stent in this position. This got stuck in the original stent during the procedure, but they pulled it free with some force and then deployed it successfully.
Just over one year later in August 2012, I had symptoms again, and they used pressure testing during an angioplasty which showed that I had restenosis, ie my body was filling up the stented area of the artery. They used a drug-coated angioplasty balloon in the area of my existing stents to clear this.
In May 2019, my symptoms began to return again. In July, an angiogram showed I had bad restenosis in the stented area of my LAD, and a new blockage forming in my large obtuse marginal coronary artery (OM1) of about 65 - 70%. My cardiologist recommended I now have a LIMA (left internal mammary artery) to LAD bypass and he referred me to a surgeon at the Royal Brompton Hospital in London. By now I was no longer on private health, but the NHS in the UK is actually extremely efficient for major cardiac surgery, and my cardiologist was able to pick the surgeon he wanted.
On 7 Oct 2019 I had doublecoronary artery bypass graft surgery. They carried out a LIMA bypass for my LAD and a standard vein bypass for my large OM. A LIMA bypass redirects the left internal mammary artery, which feeds the chest wall from the aorta, directly into the LAD, below the blockages. See diagrams below
I wrote the following account for a relative who had valve replacement and bypass surgery in February 2020. It was intended to explain to him what the surgery may be like before he had it, based on my own experiences:
CABG (Coronary Artery Bypass Graft) Surgery – October 2019
Regarding my bypass surgery last October, I had never had any surgery under general anaesthetic before, although I have had two angiograms and three angioplasties. In addition, right up until a few days before, I thought I was having minimally invasive heart surgery, so I was shocked to find out I was actually having a full sternotomy procedure. This all made me rather nervous beforehand, but I need not have worried – these operations are almost routine now, albeit still major. A bigger issue is cancellation, as this is quite common for elective patients. I was cancelled once, but my cardiologist made sure it did not happen again. If you are medically interested, my surgery was a LIMA to LAD bypass and a standard vein graft to the large OM. The LIMA to LAD was the driving reason though.
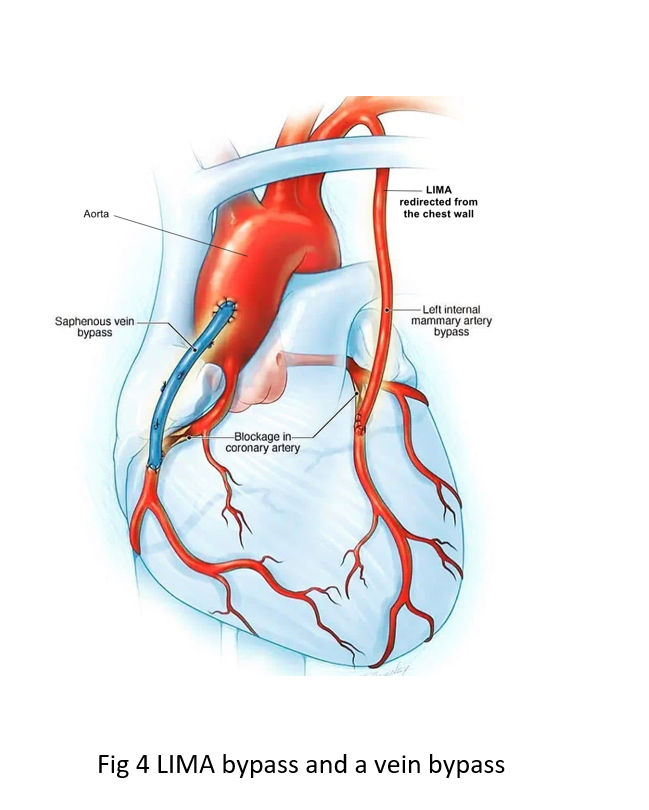
LIMA bypass and a vein bypass
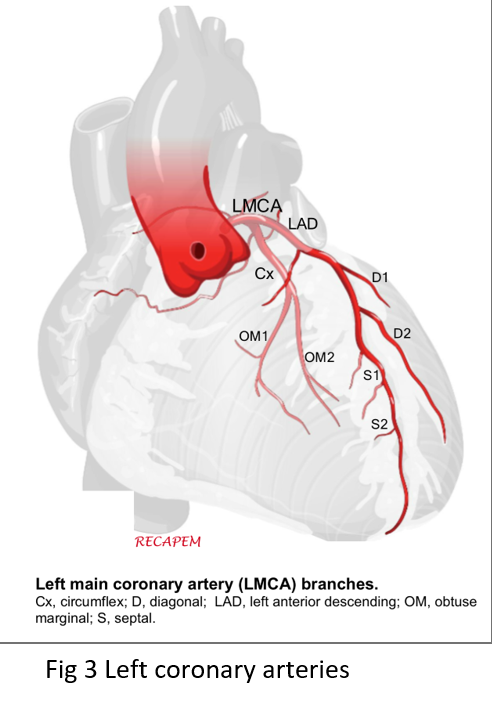
Left coronary arteries
The pre-op process is straightforward. Shaving of chest, legs and arms for access to blood vessels they may want to harvest, nil by mouth overnight, and a couple of tranquilizers an hour or so before going in. After I was put under, the next thing I recall is being woken by my surgeon asking if I wanted the breathing tube taken out. I couldn’t even feel it, but I just said yes anyway.
I felt reasonably OK immediately afterwards and I was replying to phone messages and eating within a couple of hours. The first night was in the ‘recovery’ unit, which is effectively one-to-one intensive care. You have a morphine pump for pain, but I hardly used it at first – they put local anaesthetic in your chest during the surgery and I am very sensitive to this. It should wear off in a few hours, but in my case, it was over 30 hours! Then I did need my morphine, but the pain was still manageable! If you don’t get on with morphine, there is an alternative, but I think that is more for patients who have a particularly bad reaction to it.
I soon found I was nauseous though and they had to give me anti-sickness medication for the next 2-3 days. It was caused by a combination of the general anaesthetic and the morphine, and I didn’t eat much more until this subsided.
The next morning, I was moved to the High Dependency Unit (HDU). Here they got me to stand up and walk a bit. The highly skilled nurses keep monitoring your blood gases and blood chemistry and top you up with fluids, vitamins, minerals, other meds, etc, and oxygen as required. There is a large venous line in your neck with multiple tubes for this, as well as a venous and an arterial line in your wrist and hand. The catheter was still in place too, but this was not uncomfortable. There are also two large plastic drain tubes inserted below the bottom of your sternum and a third smaller drain tube there too. These tubes make standing and walking painful and it was so much better when the two large ones were removed on the third day, along with the catheter. Removal of the drains is quite painful, but thankfully quick. The final, smaller drain tube is removed closer to going home and this is also a little painful, as it is longer than they make out.
Due to the chest wound, you tend not to breathe deeply enough, so they get you to do some simple breathing exercises and show you how to cough holding a rolled-up towel on your chest to minimise pain and movement. I continued to use this towel method for coughing for the next 2-3 weeks.
Later on, during day 3, I walked myself to the normal ward where I stayed until release on day 5, which was a day early, as I was deemed well enough to skip a day. While on the main ward you have a trolley stand with drip bags hanging from it, plus an external pacemaker, heart monitor and a drain bottle for the remaining drain tube in your chest. It takes a bit of care and practice to wheel this all around safely and you are somewhat knackered after the surgery, which after all is a major procedure. In my case they removed most of these things within 24 hours and just left the small drain, which made moving around much easier. The thin wires going to my heart for the pacemaker were left in place and trimmed just below the skin. I believe that some surgeons still remove them completely, but there is a small risk of damage to the heart in doing this, so many now leave them in place.
There was a man in his early 70s opposite me who had a valve replacement and he was doing really well. He seemed to recover faster than me and was up and about very quickly. However, they didn’t send him home early, presumably because of his age and what was done.
I should add that I was moved bays a couple of times as it is very busy on these cardiac wards. The nurses were stretched, but I spoke to a few who said they had transferred to quieter roles, but soon returned because they missed the action.
As to getting home from Royal Brompton, I had originally planned to use the trains, but I definitely felt too delicate and vulnerable for that, so used an Uber Exec instead. For me, I was much better off at home – for one thing I could sleep without being woken by the constant noise from heart monitors and doors slamming, etc – but the first week or three is still quite tough. They only gave me standard paracetamol for pain, and although this helps if taken regularly, I could not get through the first weekend without taking something stronger. Luckily I have Co-codamol 500/30 for neck pain at home, so I used this for a few days. Otherwise you need to contact your GP.
A couple of other things to watch out for. They harvested a vein from my leg for the second bypass and this was done very neatly endoscopically, so there was no big wound. However, they forgot to remove my dressing and tell me how to manage it. There were also some clear stitches protruding, so I called the hospital and was told to see my local GP nurse, who then told me these dissolve anyway!
Regarding medication, I have been on a set of cardiac management pills for 13 years (2006 - 2019), but if you haven’t had them before, you may find that the onslaught of new medication affects you both mentally and physically. They also forgot to put one drug in my take-home medication pack, so I had to call the hospital to confirm and then get it from my GP. Similarly, my GP surgery made a couple of errors on my updated repeat list which I had to sort out myself.
Remember also no lifting for the first six weeks, and then not much. I forgot on Day 3 in the hospital and lifted my heavy travel bag, but the surgeon’s registrar said not to worry, as it takes a few heavy lifts to do any real damage.
I have said little about the chest wound. Mine was done extremely neatly and the cut bone appears to have been wired up very well. It caused me some pain in the first week or two and remained sore and uncomfortable for several weeks more. Even now in week 13 it is still a bit sore and slightly numb, as is my leg, but it is not a problem.
UPDATE (up to 2022)
Since surgery, I have been healthy. However, the lower part of my scar has thickened (keloidosis) and it can be a bit irritating. In February 2020, I had a stress echocardiogram and it showed that my heart was working well.
In January 2021, I had a strange event which was never diagnosed. It was linked to tree cutting for two days with heavy equipment. I had unusual chest pain which was a mixture of musculoskeletal pain and angina, and the hospital found that my troponin levels were creeping up above normal, which is an indicator of a heart attack. The levels were still relatively low, but they gave me the medication they usually give people for a heart attack. I then recovered quite quickly and went home the same day.
Information for general purposes only; not medical advice—seek professional healthcare guidance if needed.
© 2026 All rights reserved. Links permitted and encouraged; no reproduction or reuse without permission.